The following interview was originally published on Daily Medicine, a blog full of quotes, ideas, lists, and general knowledge. Check it out for your daily dose of medicine!
In the first “Medical Student Sunday” of 2016, Daily Medicine Blog welcomes fourth year medical school student Marc Katz! Many of you have asked me for a look into a Caribbean medical school and now the chance has come to meet a great student from Ross University. Soon he will be matching into a residency spot and I can not wait to congratulate him. Until then, peek into his life through this candid interview:
Who are you to the world?
I’m a first generation American born to South African immigrants, a fourth year medical student currently finishing up my last few interviews for residency in internal medicine with plans to pursue a fellowship in cardiology. I also run a blog, MyKatz, where I advice pre-med and medical students about the hidden curriculum of medical school and try and teach others through my mistakes and experiences. My hope is that I can one day I can use my blog as a medium to educate my patients and expand their understanding of disease, health, and wellness. When I’m not in the hospital or library you can find me playing basketball at the gym, playing Call of Duty, finding a new show to watch, or reading a new book in the park. Right now I’m finishing up Scar Tissue by Anthony Kiedis and the next book on my list is The Man in the High Castle. My cousins told me that the show the book is based on is really good so I want to try and read it before I watch it. It’s the same way that I got into Game of Thrones. Except for GoT I binge watched the first two seasons and then didn’t want to wait for the next season to come out next year so I just read the books instead.
What has been your journey to medical school? (Were you a traditional or non-traditional student? Did you always want to be a doctor? Etc)
I went straight from undergrad at SUNY- Binghamton to Ross University School of Medicine. I didn’t realize I truly wanted to pursue medicine until my junior year of college so unfortunately my GPA was ever so slightly below average when I was applying. Ross accepted me for the fall semester so I jumped at the opportunity to start my medical career.
Although my grandfather was a well-respected pediatric surgeon in South Africa I was never really pressured into pursuing medicine. It just kind of happened. I blame the years of watching ER growing up. Fun fact, Christiaan Barnard, the man who performed the first successful human-to-human heart transplant in the world, was my grandfather’s resident!
What is it like attending a Caribbean medical school? (A lot of students ask me this and I would love a more detailed answer to this particular question)
I loved attending Ross University! It was an amazing experience to study abroad in such a beautiful country. Sure, we had some annoyances. Dominica’s water filtration system was gravity. So when it rained heavily it would trudge up mud and our water would be turned off. I remember walking home from the gym and it started to pour. Lo and behold when I got home I had no running water. Luckily I prepared for this situation and I had a nice shower with bottled water the day before my exam. But it’s not all bad. My strongest memories are those spent with the friends I made on the island. Attending medical school in Dominica is like going to war because only those who experience it can truly understand what it’s like. I spent almost every waking moment with the friends I made on that island for four semesters straight. I seriously wouldn’t have gotten through medical school without my island family and I’ll love them forever for it. Just please don’t tell them I said that. It would be sooo embarrassing if they knew.
To you, what is the hardest part of medical school?
Hell, where should I begin? I almost appreciated being on a literal and figurative island during my first two years of med school. We had no distractions and nothing to do besides study…and maybe drink. So focusing on my studies wasn’t difficult but figuring out how to study was. It took me a few weeks to realize how I study best and it was my first major hurdle in medical school. It’s also been the basis of a few blog posts I’ve authored, like How To Study In Medical School, because of how important it is during any graduate education. The next part, actually studying, is even worse.
You have an average of five to six hours of lecture material every day followed by five to six hours of studying every day. It sucks and there is no shortcut. Thankfully I’m a huge nerd and I enjoyed learning about most of the material, but let’s be real…nobody actually enjoys memorizing the enzymatic steps of the Kreb’s cycle.
What is a normal day like for a 4th year medical school student?
I actually wrote a blog post about the day to day life of a third year which you can check out here, The Day To Day Schedule of a Third Year, but I’ve never been asked about fourth year before because there really is no ‘normal day’ of a fourth year medical student. The day-to-day life of a fourth year really depends on the rotation and the individual. I’m willing to bet someone who is going into a surgical residency might have a completely different clinical schedule than I do. I wanted to tour everything internal medicine has to offer so my fourth year schedule has been cardiology, nephrology, hematology & oncology, a medicine sub-internship, gastroenterology, pulmonology, and I’ll be finishing up medical school with an HIV/AIDS elective. Some rotations work you hard and keep you long hours while others let you enjoy your last year of freedom before residency starts. So in that regard fourth year is kind of like third year…you’re just slightly less of an idiot.
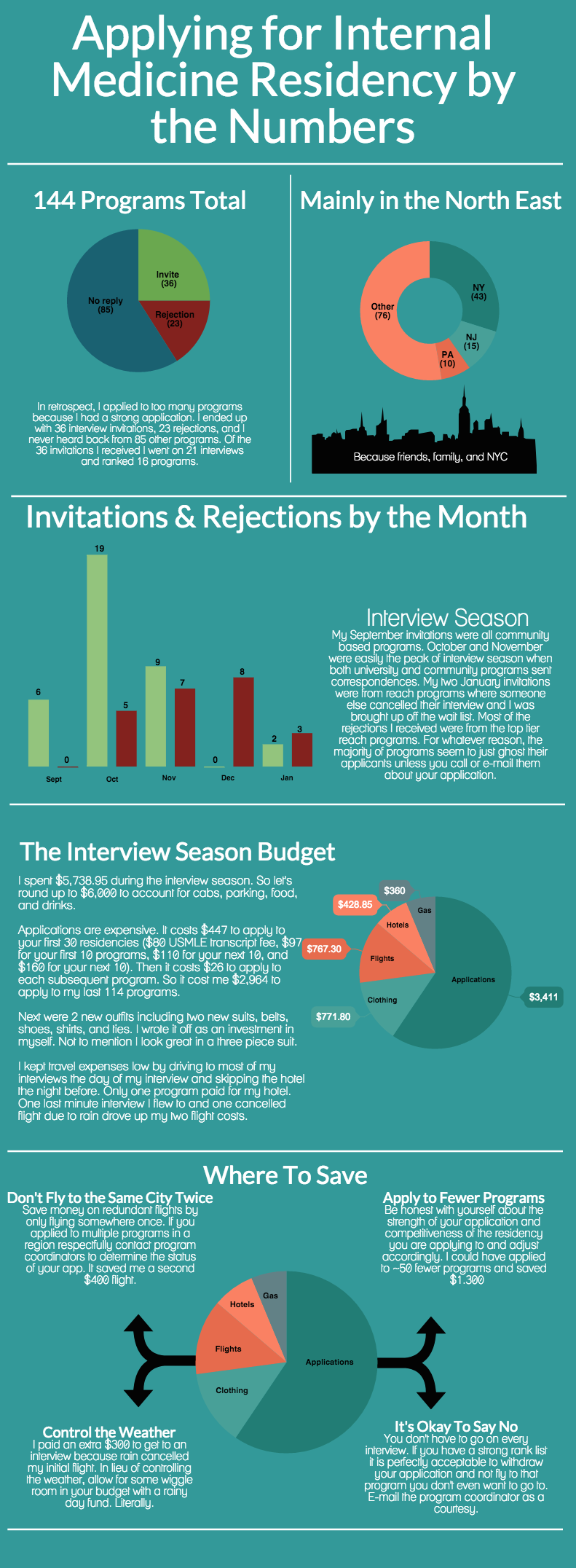
Fourth year also includes interview season and it leaves you tired and drained during November and December. That being said, my fourth year has been my favorite year of medical school so far. I’m not constantly anxious about having to go study for step one or step two and there aren’t any more tests, just patients. So I finally get to be self-driven about studying and pursue learning about what interests me. I’m just really excited for residency to start. And for my trip to South East Asia with my friends before residency starts.
What is the best advice you ever received?
Never yell at the food staff before you get your food and always pay for your date’s meal. Though I have a feeling you meant it with regards to medicine. If that’s the case then I must admit that the best advice I’ve been given isn’t all that original. I distinctly remember two different people telling me the same advice for two different reasons.
As a third year I was growing frustrated in my attempts to impress my attending whom I wanted a strong letter of recommendation from. And as a fourth year on my medicine sub-internship I was growing frustrated by my patient’s family’s indifferent attitude about the medical care of their loved one. In both instances my roommate and senior resident, respectively, gave me the same advice that was applicable to both situations. They told me to provide and coordinate the best possible care for my patient.
Instead of trying to read my attending’s mind I simply focused on taking care of my patient. I did what I could to make someone feel better everyday. I learned that I can sleep at night knowing that at the end of the day I did everything in my power to take the best care of my patient to the best of my abilities.
What qualities in a shadowing pre-medical student impresses you?
The most impressive pre-med students are those that are awake. Seriously, if you’ve got a heartbeat, a smile on your face, and a skip in your step then you’re already better than half the kids I’ve seen. I remember my favorite pre-med student that was shadowing a surgeon I was working with for the month. During surgery she would diligently write down notes about things she wanted to look up later. She would come back with information that she looked up and asked us follow up questions. When we were waiting for rooms to be cleaned she asked to go watch other surgeries. She showed us that she wanted to be there by being engaged. She was visibly excited to be there and it made my day more fun when she was around. They are the same values and characteristics that make for a good medical student. You can read more about what qualities in a shadowing pre-medical student impress me the most in my blog post, Premeds: How To Shadow Like a Boss.
What do you like to do for fun?
Does brunch count as a hobby? Well besides drinking coffee, Bloody Mary’s, and mimosas, I also like to visit my brother at Barclay’s Center where he works and try to go to as many Brooklyn Nets and Islander’s games as I can. I’m also currently trying to knock out my New York City bucket list just in case I don’t match here. By the way, turns out the MOMA closes at 5:30pm during the week in case you wanted to go. Made that silly mistake last week. Still trying to find time and someone to go to the top of One World Trade Center with.
Do you have a few tips for medical school students & premeds?
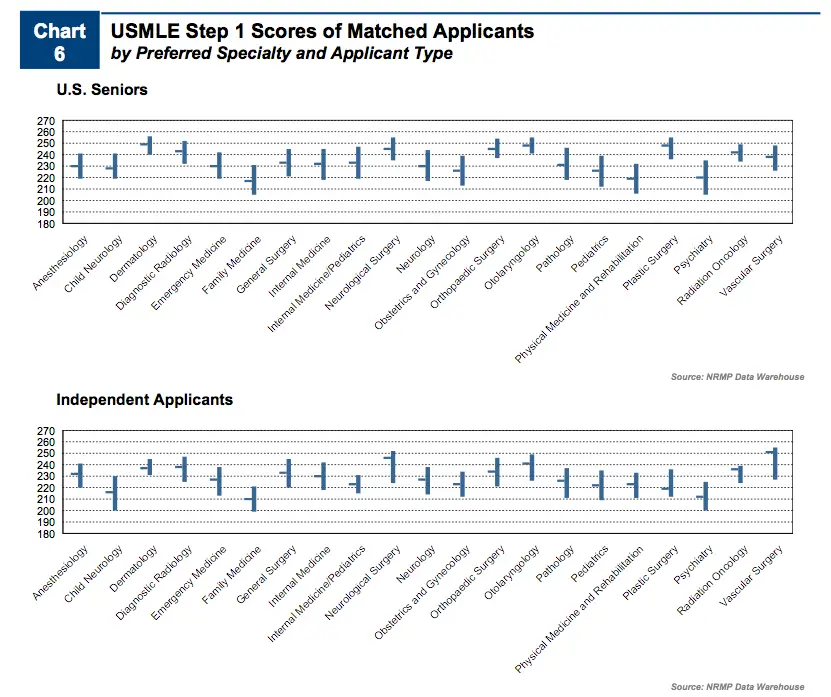
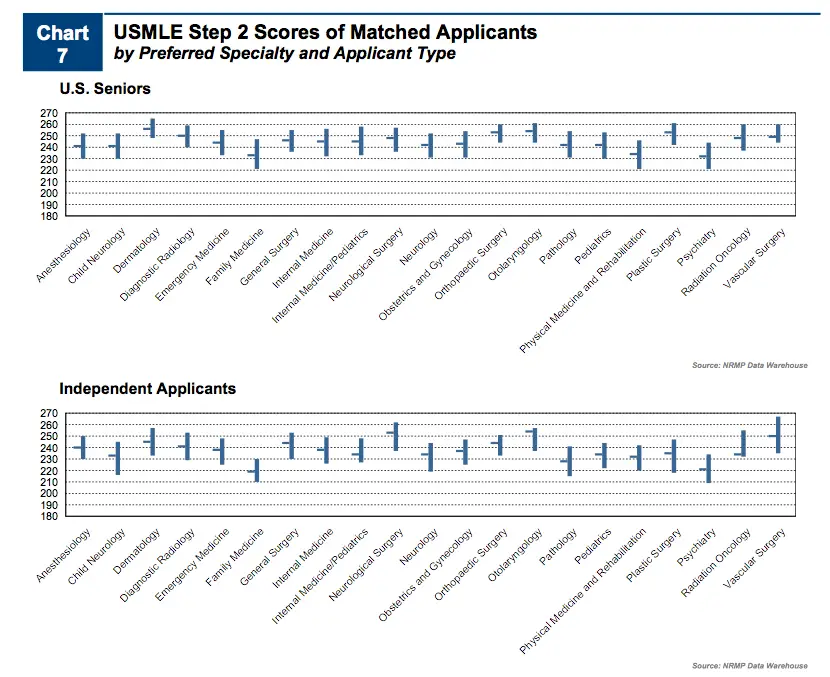
I have too many tips for medical students and premeds! I could preach for days about mistakes I’ve made en route to medical school and how to avoid them as well as how to succeed in medical school. But I do have one real piece of advice for premeds and medical students alike and its not going to be very popular with your friends or family. It is to be selfish. Nobody else is going to make your medical education as their number one priority. That is your job. You are going to miss birthdays, anniversaries, weddings, holidays, parties, and average day to day moments that your friends and family will spend together. You on the other hand should be in the library or hospital studying. As I’ve stated before in a post about The Match, you need a strong step score in order to get past residency program filters and the only thing standing in your way is you. So be selfish and go study.
That being said, if anyone reading this has a more specific questions you can always comment on my blog and ask me a question here or tweet at me at @MarcKittyKatz and I’ll do my best to get back to you as soon as I can!
If you are in a relationship, how do you handle balancing school and a committed relationship?
I am probably the worst person to ask about this…because science is my lady. Just kidding! My life isn’t that sad. I am currently single but I can comment that having a relationship during medical school is totally doable. Tons of classmates of mine met their significant others on the island and during rotations. In my humble opinion, you just have to be honest with yourself and your partner about your med school obligations and make your relationship a priority. It’s just like when people say ‘they don’t have time to exercise’. Nobody in medical school has an extra hour or two in their day but you can make time to exercise and you can make time to date and have a relationship. You just have to make it a priority. I mean, it’s not like it’s going to get any easier in residency. And when in doubt, swipe right.